



Beat the Flu: Essential FAQs
Expert Answers on Prevention, Treatment, and Symptoms


No experience like first-hand experience with the flu to make this a timely (and maybe more nuanced) message. Thanks to my trusty toolkit (we’ll get into it later), I’m on the mend! Here’s the revised information with more facts, less fever dream.
The 2024-2025 flu season is hitting the emergency departments hard, especially the pediatric emergency department. Currently, approximately 33% of ED visits for children (0-17 years) are due to flu or influenza-like illnesses. There have been an estimated 33 million infections, approximately 430,000 hospitalizations, and 19,000 deaths including 86 in children. This season is proving to be exceptionally challenging compared to the past decade. We think the peak is near, but we've compiled an influenza FAQ to help you and your family navigate this difficult time.
For near real-time updating and expert data crunching, head over to Your Local Epidemiologist or Force of Infection.
Nuts and bolts of the virus itself
What are the Hs and the Ns?
Flu viruses are orthomyxoviruses which are enveloped and have special surface proteins. The surface glycoproteins Hemagglutinin and Neuraminidase help the virus replicate.
Hemagglutinin helps virus attach to host cells; after the virus goes ham replicating inside host cells, neuraminidase helps newly made virus get released and infect additional cells.
There are 18 subtypes of hemagglutinin and 11 of neuraminidase, and viruses are named for their subtypes.
How are flu strains named?
Three kinds of influenza affect humans: Influenza A, B, and C (the creativity!). A and B are the ones you see most often (C causes milder illness) and are named scientifically according to convention. For A, it’s based on type, location, year and subtype (ex: A/Ohio/2021/H3N2) and for B there are two lineages (Yamagata and Victoria).
What's the difference between seasonal flu and a pandemic?
The virus adapts by mutating so it can more effectively infect.
When the mutations are on a smaller scale, that is antigenic drift; these cause seasonal outbreaks.
When there are major changes, or antigenic shift, we get pandemics.
Historically, Influenza A has been the cause of global pandemics. This is because Influenza B shifts more slowly and is mostly in human hosts, rather than animal reservoirs. You can see why everyone is very nervous about the spread of avian flu to cat, cow, and human hosts!

Stop the spread: Understanding transmission
Why does flu season happen?
While flu viruses circulate year-round, they peak in winter (Oct-Mar in the Northern Hemisphere, Apr-Sept in the Southern). In tropical climates, flu can be present year-round.
How is it transmitted?
Via droplets (coughing, sneezing, talking), contact (touching sick people, sick tissues like boogery noses you have to wipe, and surfaces covered in virus), and aerosol. In my case, despite incredible caution at work and in public, as soon as I saw friends with tiny germ monsters from aged 1 - 5 years, I was felled.
When are you contagious?
Even several days before getting symptoms and knowing you are sick, virus can be detected and you can be shedding virus and thus contagious.
You are most contagious with highest viral shedding within 24 hours of symptoms, with the first three days of being sick being the worst.
Because kids are the germiest, they can have longer shedding periods and higher viral loads than adults.
What if someone in my house has the flu?
Be very careful, you are likely to get it - there’s about a 40% risk of getting it from household contacts.
When can I return to school/work?
Of course, this is an individual decision best made with your doctor and your family, but the recommendation is at least 24 hours after being fever-free and after symptoms improve.
Who is most at risk?
Children <5years old, people older than 65, pregnant people, people with chronic medical conditions, also people with lung conditions or who are on immunosuppressants

Influenza symptoms and diagnosis
What are the symptoms?
Sudden fever, chills, headaches and body aches, and general misery. In kids, there can be more stomach-bug type symptoms than in adults with nausea, vomiting and diarrhea.
How do you diagnose it?
When the flu is widespread, suspect it. You don’t always need a swab.
So then why is a test sent if we already suspect it?
We live in communities and sometimes need to know. This can be because of implications for return to daycare or school, cohorting people with the same virus during hospitalization, or for planning visits to loved ones who are at higher risk of complications.
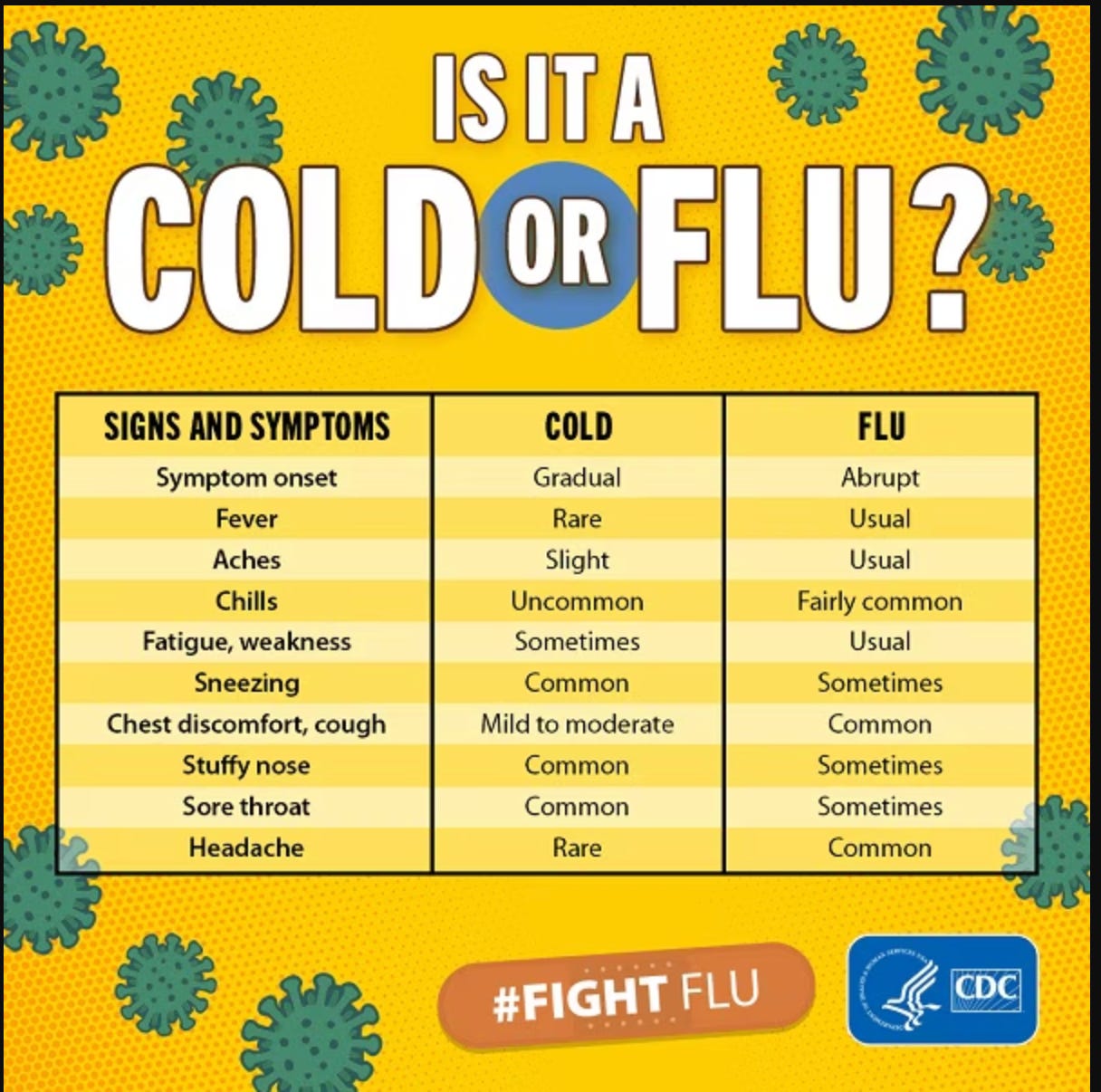
How can I tell if it’s a flu or a cold?
This is a tough one. They are caused by different viruses (influenza vs. rhinovirus). Symptoms can overlap. A lot of people assume if a cold is annoying enough it’s a flu, and in some languages the same word is used for both.
Generally, colds are milder, and are more likely to have upper-respiratory tract symptoms (runny nose, stuffy nose).
The flu tends to have more generalized symptoms like body and muscle aches, worse fever, and a higher risk of lower-respiratory tract symptoms (lung problems as opposed to nose problems, which are upper respiratory tract).
When should I worry about flu complications?
Ear infection (otitis media): severe ear pain after 4 days.
Pneumonia: especially in children under 2. This is when you get a bacterial co-infection in your lungs on top of the flu. Think about this if your fever was improving and then all of a sudden gets much higher again.
Dehydration: not urinating more than twice daily. Electrolyte drinks can help in older people; in younger kids and babies, you may need IV hydration.
The flu is serious; the most severe complications can involve brain dysfunction (encephalopathy) and even death.
What's a unique symptom in children this season?
Viral myositis: severe muscle tenderness (often in legs), toe-walking, pain with calf flexion.
Muscle breakdown can occur, potentially affecting urine. In this case the urine will look dark - talk to your doctor if this happens, as they will need to look carefully at kidney and muscle function.

Flu Prevention: Your Vaccine Action Plan
How can I reduce my flu risk?
Social distancing, hand hygiene, and staying home when sick are key. Masking when in public spaces with lots of other people.
When and who should get vaccinated?
Everyone over 6 months unless you have a specific medical reason not to get vaccinated. October is ideal since it’s the beginning of flu season, but it's never too late, including now (especially if you are at risk or live with someone who is).
Priority: pregnant people, those over 50, those with chronic conditions, nursing home residents, immunocompromised individuals, and caregivers of young children.
But the flu shot gave me the flu!
We hear this all the time. Probably not, or at least don’t blame the vaccine! What happens to a lot of us, especially if you have children, is you sat in a germy place (like a doctor’s office or hospital) where lots of germy contagious people who are bad at wiping their noses and coughing into their elbows gave you a virus, maybe a cold, maybe the flu. Remember, flu can exist on surfaces and people can shed it before they feel sick.
Additionally, as your immune system responds to the vaccine to build those little virus fighting antibodies, you can get a constellation of symptoms including headaches, fatigue, muscle aches and mildly elevated temperatures - sound familiar? This can be easily confused for influenza infection. Frankly, I don’t mind feeling these symptoms because I know that I’m having an appropriate response and my immune system is gearing up.
Why does the flu vaccine change yearly?
In order to keep up with the anticipated changes in Influenza A, which mutates rapidly. New vaccines are created based on WHO strain surveillance (good job, WHO!).
Of course, there is both data-driven surveillance and some guess work involved; different years’ vaccines thus have different success rates. The virus is wily; pandemics happen when a new influenza A strain spreads rapidly with little immunity or vaccine protection.
What are the vaccine types?
Egg-based: Standard dose (aged 6 months+), high dose (aged 65+), recombinant HA (aged 18+), live attenuated nasal spray (aged 2-49, more details below).
Non-egg based: Recombinant and cell culture vaccines.
What if you or your loved ones hate needles? Nasal flu vaccine is for ages 2-49, non-pregnant, no significant chronic medical conditions BUT not for children aged 2-4 who have wheezed in the last year.
GREAT NEWS: FluMist was approved for self-administration in September 2024 - will likely be available for the 2025-2026 season
Bottom line: Consult your doctor for the best option, especially with chronic conditions.
Can I get multiple shots at once? Yes! Flu, COVID-19, RSV (data ongoing), and pneumococcal vaccines can be co-administered at different injection sites.
Why do some kids need two flu shots?
Children 6 months - 8 years need two doses (4+ weeks apart) if they haven't had two in a previous season in order to build up their immunity. Afterwards they can have one dose a season like the rest of us.
Influenza Treatments & Symptom Management
Antivirals: Do they work?
Yes, for both treatment (lessening symptom severity) and post-exposure prophylaxis (see below).
Neuraminidase inhibitors (like Tamiflu) reduce flu risk by 50-80% once exposed.
For treatment, antivirals must be taken within 48 hours of symptom onset. If taken later, there is limited efficacy in shortening duration of symptoms.
What is post-exposure prophylaxis and who is it for?
Preventative medication after exposure to the flu to stop infection.
For those who are at high risk of complications (very young children, the elderly, those with lung problems, pregnant people, those with immune compromise).
What are the side effects of antivirals?
GI issues (nausea, vomiting, diarrhea), headache, dizziness.
Rarely, neuropsychiatric symptoms (self-injury, delirium). If you experience these, stop the antiviral and talk to your doctor. Some studies have suggested a higher risk in children, but this has not been confirmed with high quality evidence. If there is a history of significant psychiatric illness, discuss with your doctor if the benefit outweighs the risk.
Who should get antivirals?
High-risk individuals, those during the first 2 weeks post vaccination, severely immunocompromised or those who can't be vaccinated.
Consider for outbreaks in institutions (long-term care, transplant units, neonatal units).
What if I am pregnant?
Sorry about the timing! There’s never a great time to get the flu, and this is absolutely a bad one. You have enough going on.
You will need to take Tamiflu/Oseltamivir.
If you deliver while you are contagious, you will need to wear a mask around your baby to try to prevent exposure. In some hospitals, your baby may be placed in an incubator.
Your household contacts should also wear a mask around the baby (we just assume they are also germy and err on the side of caution).
You can still breastfeed if you want! Just wear a mask.


Influenza Symptom Management: Your Home Toolkit
We will be using brand names but thanks to the wonders of patent law, many of these medications have store-brand generics that are just as effective and can save some dollars.
What medications help with fever and muscle pain?
Acetaminophen (Tylenol) or NSAIDs (ibuprofen, naproxen, Motrin, Advil, Aleve) are excellent at symptom management. You can alternate between the two every 6 hours because the body processes them differently.
For your child, asking their pediatrician for appropriate weight-based dosing can be helpful.
Avoid salicylates (aspirin) in children due to risk of Reye syndrome. We are not sure exactly why this happens with influenza infections (or chickenpox), but it can cause damage to the liver and brain.
Avoid combination cold medicines (cough medicine + acetaminophen or ibuprofen (Dayquil, Nightquil)) to prevent accidental overdose, especially in children. It is easier to keep track of your dosing of active ingredients if they are the individual medications.
What helps with nausea, vomiting and diarrhea?
Nausea/vomiting: ondansatron (Zofran) is the most common. It comes in an oral dissolving tablet (ODT) so it’s harder to vomit up. It does need a prescription from your doctor.
Diarrhea: bad humors (and bad poops) are generally better out than in. Therefore, loperamide (Imodium) and other anti-diarrheals are not recommended for children.
What helps with congestion and runny nose?
1. First the drugs:
Pseudoephedrine (Sudafed, the good stuff, behind the pharmacy counter, have your ID ready):
Children: use weight-based dosing; adults: use the package insert
Note: May cause elevated heart rate, high blood pressure, decreased appetite, dry mouth, urinary retention, dizziness.
Avoid in first trimester of pregnancy.
There is some penetration into breastmilk but it is at a level considered safe.
Oxymetazoline aka Afrin (nasal spray)
Adults: 2-3 sprays per nostril twice daily.
Children >6 years: 0.05% solution, 2-3 sprays per nostril
Can use for 3 days, but do not go longer than that or you will have rebound symptoms (the most epic runny nose, like a faucet).
Fluticasone aka Flonase (nasal spray):
For runny nose during illness or for post-viral lingering cough (which is sometimes due to post-nasal drip): 2 sprays per nostril once daily.
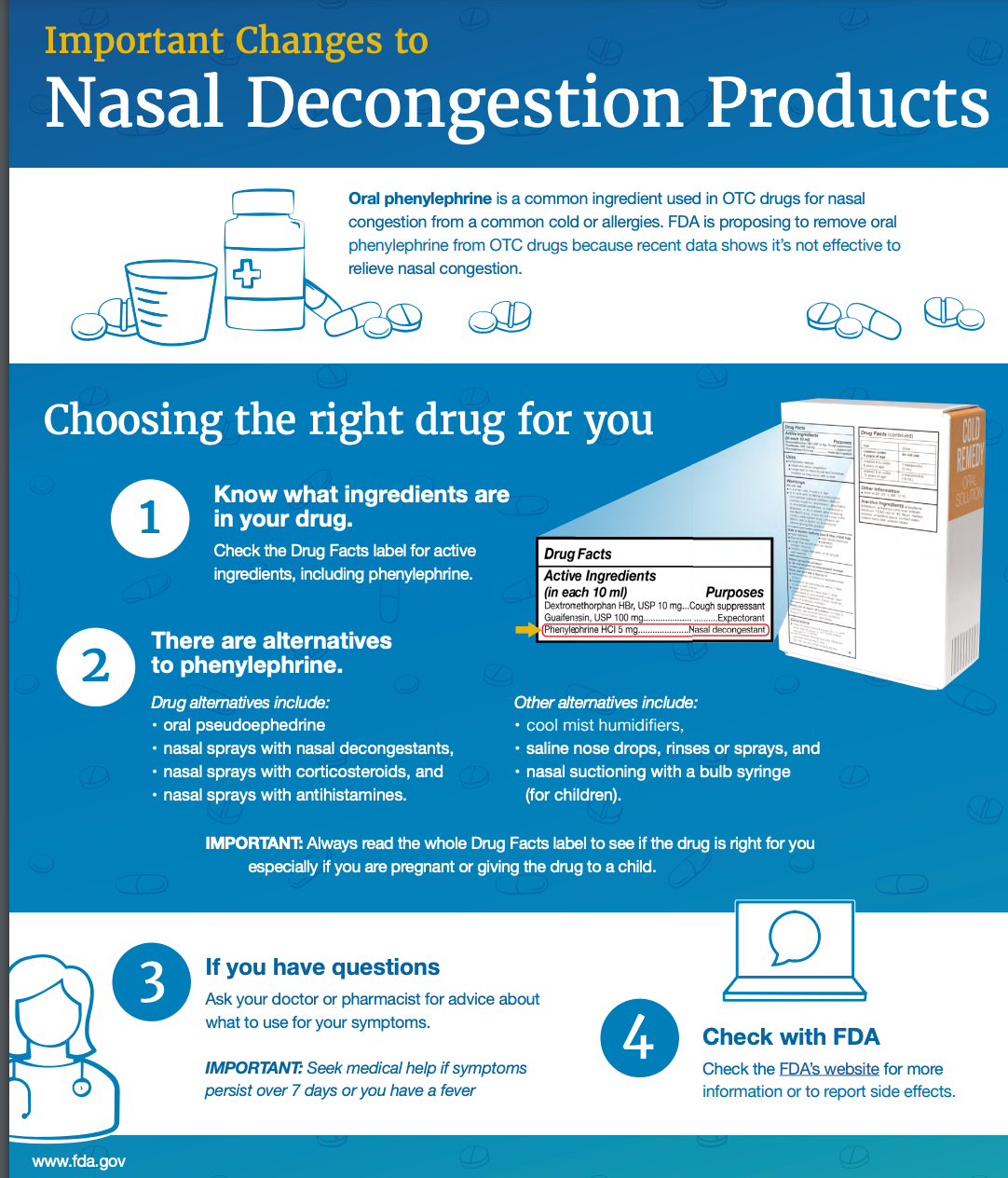
THROW OUT YOUR PHENYLEPHRINE-CONTAINING MEDICATIONS
FDA: Current data do not support oral phenylephrine use. It doesn’t improve symptoms reliably and has side effects. If you’re curious, check out the notes from NPR or from the FDA directly.
Supportive care that should be in your kit:
Neti Pot or saline rinses: It is very important to only use your Neti pot with distilled water, sterile or boiled water but this can be a game changer for nasal congestion. It is also both gross but deeply satisfying to clear out all the mucus.
Lotion-enhanced tissues: save the poor snouts! With the amount of nose-blowing, you’ll be thankful to have these on hand. If you don’t have that, a dollop of good old vaseline at the nostrils can help humidify the air and protect the skin.
Honey: has been shown to help with natural cough suppressants (that’s why many children’s cough medicines are honey-based) and if you use local honey, the exposure to local allergens can be helpful in reducing seasonal allergies over time (bees are magical!). Can be soothing to sore throat as well.
Avoid in kids younger than one year old - this is not safe! (There is a risk of infant botulism).
What about natural and complementary remedies?
There are all manner of concoctions being pitched online to help both with prevention and improvement in flu symptoms. We would like to point out that companies such as Airborne, Zicam, and Oscillo have all been subject to lawsuits over deceptive and misleading advertising and marketing about the efficacy of their potions in preventing and improving symptoms.
The supplement industry remains unregulated by the FDA so it is often difficult to know if you are actually getting the promised substance and whether the claims they make are correct. Many things have been suggested to improve the immune system: echinacea, elderberry, garlic, Vitamin C, Vitamin D, zinc. Unfortunately there is limited large scale data to suggest significant improvement in the preventing or treating the flu. Sorry! It would be great if they worked.
Want to impress your trivia team with some truly wild medical lore? Let's talk oscillococcinum. Maybe your algorithm has tried to convince you this will help your flu, or any number of other illnesses. What is it? Well, it's a homeopathic remedy, which means it's based on the idea that 'like cures like.' So, if something causes symptoms, a tiny, tiny bit of it will cure you. (Confused? Yeah, us too.)
Now, to make oscillococcinum, you take duck liver and heart, ferment it, and then dilute it... a lot. Like, imagine diluting a single drop of duck soup into the entire ocean, then diluting that 199 more times. At that point, it's basically a sugar pill with a faint memory of duck. Does it work? Science says nope. We say, save your money for actual medicine (or at least, tastier snacks).
For those of you who've already been initiated into the 'Flu Club' this year, we hope your couch is comfy and your tissues are plentiful. If you've somehow managed to escape the clutches of the influenza beast, kudos! Keep up the good work (and get vaccinated, seriously). We're all looking forward to spring, when we can hopefully enjoy more sunshine and norovirus (just kidding). Fingers crossed, and may your immune system be ever in your favor.
As we navigate this challenging flu season, remember we're in this together. We're committed to providing you with the best information and care possible. Now, we'd love to hear from you. How has the flu season impacted your family or community? Share your experiences in the comments below.
Disclaimer: The content provided in Couch Nap is for educational and entertainment purposes only. It is not intended as medical advice, diagnosis, or treatment. It does not establish a doctor-patient relationship. Always consult with your healthcare professional regarding any medical concerns or decisions. The views and opinions expressed here are our own and do not represent the positions, policies, or opinions of our employers or any affiliated organizations. While we strive for accuracy, the information presented here may not apply to your unique situation.
This is an excellent summary. Thank you.