



How To Be a Patient, Part 2: How to Deal With the Emergency Department
What to take, what to ask, and what to do after going to the ED.

Welcome to How To Be a Patient, Part 2.
In Part 1, we discussed how to organize your medical information.
Here in Part 2, let’s talk about how to prepare for patient visits to the ED/urgent care.
Stay tuned for Part 3, where we will talk about how to make the best use of visits to your physician.
The first step is to decide where you need to go.
Unfortunately, the medical system is stressed at all angles. Everywhere you go will feature a long wait time.
Patients in the emergency room are triaged by level of illness, so if you go there hoping to expedite a non-urgent test, workup, or specialist referral (as all of us have attempted at some point, self included), you will be triaged lower, likely get disappointed, and still have to wait as an outpatient.
Plus, you may have a hefty copay and an ugly bill, to boot. So the first step to avoid adding insult and overpayment to injury is to try figure out if you need the ED or your PMD.
How do I know if I need the emergency department?
We are not your doctors, so we want to emphasize that this does not constitute medical advice. What this is instead is education about things that are true emergencies, and is by no means a comprehensive list:
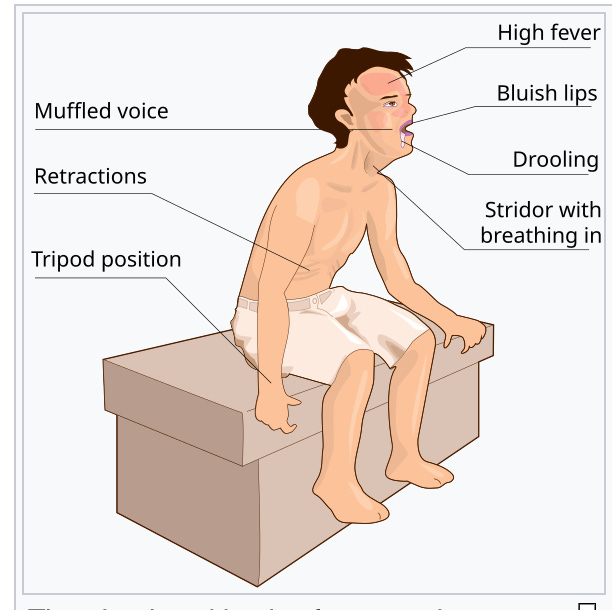
Difficulty breathing. If you can’t get through a sentence, call an ambulance.
If you need to maintain this position to breathe, called tripoding: call an ambulance.

This can happen with foreign bodies or epiglottitis. Image here. Bleeding that won’t stop
Change in mental status/loss of consciousness
Inability to tolerate anything (even liquids) by mouth
Fever IF the patient is a baby younger than 60 days, or someone immune-compromised
Broken limbs (obviously), deep lacerations
Firm abdomen that is painful to touch, especially if there is no stool and there is vomiting.
Again, this is not a comprehensive list. Chest pain, headaches, abdominal pain and vaginal bleeding can all be extremely serious (and sometimes not serious) so you have to use your judgement.
For many other concerns, it is worth calling your physician first. Many practices will have someone on-call who can ask you more specific questions, and who may even be able to look at your medical records to try to help you. The provider on the phone may be a physician or an advanced practice provider or a nurse. Some hospitals have dedicated nurse-lines for exactly this kind of triage.
✅ Action step: look up if your hospital (some pediatric hospitals do) or physician’s practice offers a dedicated nurse line
✅ Action step: put their number in your phone and take note of the hours they work (some will be staffed on evenings but not overnight)
✅ Action step: also save the number below (for Poison Control) in your phone. They are so incredible and will help you figure out what to do.
What about urgent care?
Great question. Many urgent care places can help keep you out of the cesspool that is the emergency department, especially for less severe concerns that can’t wait for your physician’s office to be open. They can be a fine place to start.
That said, they often do not have the facilities to perform and interpret many radiological studies, or patch up injuries that require many stitches. I would still start with your physician’s office for a phone call if that is an option.
✅ Action step: look up where the closest urgent care is, and what kind of services they offer
Which emergency department should I go to? What about if my kid is sick?
If you are in an ambulance, they will likely take you to the closest hospital.
If you are taking your child to the ED, and you’re going in your own car, and the distances are equal or nearly equal, go to the pediatric hospital. The available equipment, staff with pediatric training and accommodations to pediatric patients, are worth going a little further for if it is not a matter of life and death. There’s unfortunately plenty of evidence about the difference in quality of pediatric care in children’s hospitals and non-children’s hospitals. Stay tuned for a future Couch Nap about this!
✅ Action step: look up where the closest children’s hospital is. Even if you don’t have kids, you know someone who does.
What should I bring to the emergency department?
If you have a few minutes to pack, I would take:
a list of medications you’ve taken, or given your child (but you read How To Be A Patient Part 1, so this is already all set in your phone)
layers, because hospitals are freezing
a long cord to charge your phone with (hospitals have long wait times, few outlets, and crappy wifi)
water and snacks (don’t eat the snacks unless they tell you it is ok to, because that can set back anesthesia)
something to entertain your child with (crayons, book, toy - don’t bring anything precious! Things get lost in the hospital all the time. Only bring the third tier toys that you’re fine getting lost/filthy).
somewhere to take notes (your phone notes app should be plenty)
✅ Action step: pack a little pouch that has some of the above in it, and keep it near the entryway.
✅ Action step: if you are the one going to the emergency department, and you have a minute, take off your jewelry while you are at home. Hands are needed for IVs, you have to wear a gown, there are many annoying stickers and touches, and metal is incompatible with MRIs. Leave precious things at home so they don’t get broken or lost.

Pack a phone charger and a nice long cord. You won’t regret it.

What should I expect at the emergency department?
Well, chaos. Certainly not dignity. Sorry! I say that as a patient. I know Dr. Kristina is an amazing emergency department doctor and treats everyone with kindness and respect, but I just don’t count on being treated by Dr. Kristina when I go. I expect to get someone who wishes they were eating a delicious sandwich in front of their TV, or swiping on Tinder, instead of listening to my lungs.
Expect to be triaged and to be bumped if there are traumas or more acute patients. I have had to interrupt many conversations with patients in order to run to a code. I’m sorry if that happens to you! I know it feels gross and very frustrating. I will tell you what I tell my patients all the time: it is good to not be the most emergent priority in the hospital.
Expect to re-tell a million people why you came in. This feels redundant and annoying. But it is important for several reasons:
Providers have different functions (triage, assessment, consultation). They ask questions from different perspectives.
Some of the people may be trainees. They don’t always know the questions to ask, so their supervisors may need to repeat questions or ask more targeted ones.
Repeating yourself can actually be a useful redundancy that promotes patient safety, as more people can pick up different, important details, or confirm things like allergies that one person may have missed. I myself get pretty punchy (oops sorry Dr. Kristina) with people by the 17th time I have to repeat the same thing, but it’s not their fault.
✅ Action step: brace yourself for the redundancy. Try not to bite the head off of bumbling trainees. They need to get through this to one day become competent independent providers.


How to stay empowered (or try to)
This is easier to do if you have a companion with you, but as best you can, try to figure out who you saw, and what medications you received, and what interventions or images you got. It should all end up in your discharge summary, but it may not, and that discharge summary may not make it to your PMD. This is why I want you to be able to take notes in a notebook or on your phone notes app.
you don’t need to know the names of every doctor you saw, but it can be helpful to write down their specialty (e.g. if you saw an orthopedic surgeon or a dermatologist or a neurologist in addition to the emergency medicine provider)
your doctor will not have time for this, but the nurse giving you medications can tell you what medications they are and what they are for
you can ask staff to clarify what kind of imaging you are getting (not everyone knows whether they are getting a CT or an MRI, an echocardiogram or EKG)
if you get discharged, it is perfectly reasonable to ask your emergency doctor these questions:
How soon do I need to follow up with my doctor?
Are there any symptoms that mean I should come right back here to the ED?
Which medications should I take until I see my doctor?
Are there any labs or tests you did that I need to make sure my doctor knows about?
Is there anything I need to tell my doctor about this visit? What, specifically was my diagnosis?
I’ll be honest, you may get the brush-off from someone busy saying “It will be in the discharge summary.” But many times someone will tell you something like “all the tests were normal, but your doctor should know that your white count was oddly low, and repeat it.” Even if they tell you everything is normal, write that in your notebook/notes app.
✅ Action step: take a screenshot of these questions and put them in your phone; save them to a note called “for ED visits.” That way they are ready for you should the situation arise.
What happens after the ED visit?
You already know about the bill. That is very scary.
What happens in terms of communicating with your doctor is really variable. It depends on how your ED and your doctor are connected. Some EDs will reach out to the primary care physician and let them know what happened. Some will give you a little discharge summary with a write up (which, because you read How To Be a Patient Part 1, you will immediately take a picture/make a pdf of, while you are still there, because you know otherwise it will get lost) to give to your doctor and/or a copy to keep. Some practices share the same electronic record system with your ED so they may be able read notes from the ED visit and understand what happened.
But be practical. Assume the electronic communication doesn’t exist, your doctor never hears about your adventures in the ED, and they either misplace or never read the discharge summary. Advocate for yourself. Keep track of your own data. It is an extra step, but it takes literally seconds to make a pdf/take a picture of your discharge documentation, and can save a lot of time.
✅ Action step: when you are being discharged, ask for a discharge summary and immediately take the print out and make it into a picture/pdf saved on your phone
✅ Action step: after your ED visit, call your doctor and schedule a follow up appointment
✅ Action step: throw out anything that spent a long time in the ED (crayons, toys) or launder what you can. The ED is really a disgusting sewer (sorry Dr. Kristina!).
We hope this was helpful! Our next Part of the How to Be a Patient series will prepare you to make the most of doctor’s visits.
✅ Action step: One last action step: please comment on this post and let us know what else would be helpful for us to write about. Thanks for being here!
Disclaimer: The content provided in Couch Nap is for educational and entertainment purposes only. It is not intended as medical advice, diagnosis, or treatment. It does not establish a doctor-patient relationship. Always consult with your healthcare professional regarding any medical concerns or decisions. The views and opinions expressed here are our own and do not represent the positions, policies, or opinions of our employers or any affiliated organizations. While we strive for accuracy, the information presented here may not apply to your unique situation.
Great article! I've incorporated both your posts about how to be a successful patient into my article on patient advocacy:
https://drmick.substack.com/p/patient-advocacy
I’ve not had great luck with broken limbs in the ER. I try to get directly to my orthopedic/sports medicine group because that is where I will get care and ongoing follow up anyway. Sadly, I have a long standing relationship with one because I have and ride horses.
I save ER for heart, breathing, consciousness issues.